Preparing for the future
Dialysis populations around the world are rising.1,2 Although recent growth is almost completely attributable to improving survival, mortality rates remain much higher than in age-matched U.S. residents, and conventional, thrice-weekly hemodialysis may not adequately address:
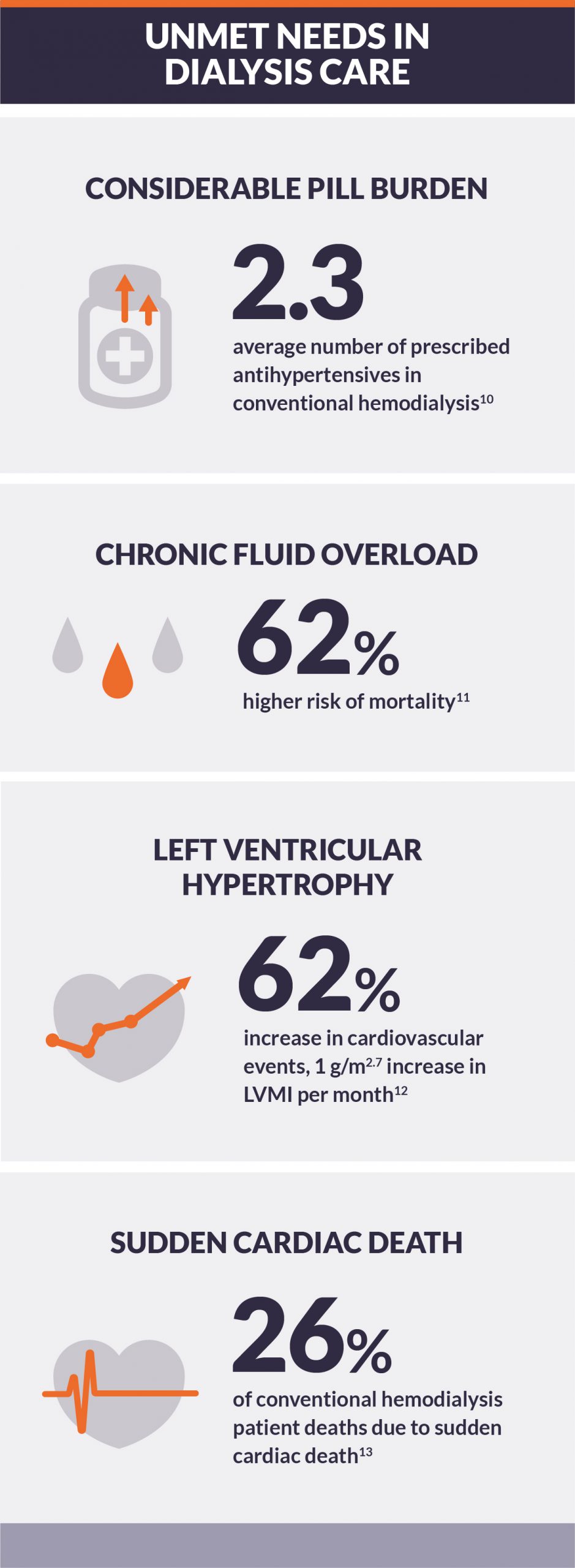
- High risk of cardiovascular morbidity and mortality3,4
- High pill burden5
- Diminished quality of life6,7
- Limited tolerability of conventional hemodialysis treatment8,9
To improve the quality of patients’ lives, intensive dialysis should be considered to address the fundamental complications that limit the long-term efficacy of conventional hemodialysis.
Impediments to increasing intensity include physicians and dialysis providers, who each must fairly present to patients and their families the alternatives that exist to normalize life with dialysis, and payers, who must recognize that potentially increased dialysis costs can be offset by decreased costs due to acute care and medications for comorbid complications.
Reviews—summarized on this website and available in full for download—present clinical evidence for intensive hemodialysis and innovative perspectives on the role that intensive therapy may play in improving patient outcomes.