In Case You Missed It! October 2024
This month’s newsletter highlights new home dialysis training tools and psychosocial and biopsychosocial considerations in patients initiating dialysis and their respective outcomes:
New continuous ambulatory peritoneal dialysis (CAPD) virtual reality (VR) patient training tool
Why understanding patient coping methods matters
Potential benefits associated with starting dialysis versus conservative care in older adult patients
Recent Findings
Authors conducted interviews with 5 nurses and 2 nephrologists, who each trained between 2 to 5 patients using a new VR CAPD patient training tool.
Learn MoreSpecial Home Dialysis Edition:
In Case You Missed It! August 2024
This month’s newsletter highlights a selection of recently published peer-reviewed home dialysis articles centered around:
Identifying Challenges
Finding Solutions
Getting and Keeping Patients Home
Home Dialysis Recent Findings
A 7-member advisory board, comprised of patients, care partners, and dialysis providers collaborated to devise lists of barriers perceived by patients/care partners and providers (clinicians, nurses, and clinic staff), respectively.
Learn MoreIn Case You Missed It! June 2024
This month’s newsletter highlights a selection of recently published peer-reviewed articles that piqued our interest related to:
Peritoneal Dialysis (PD)
Conservative Care
We hope you find these recent findings useful and of value in your day-to-day practice.
PD Recent Findings
Factors influencing renal replacement therapy modality choice from the nephrologist’s perspective
In this qualitative study, semi-structured interviews with 29 nephrologists were conducted. Using Charmaz’ constructive approach to grounded theory, four themes were identified:
Trust and belief in PD as a technique; own expertise, knowledge and team; in behavior of patient, family practitioner
Feeling of control paternalism; insecurity; prejudice
Vision of care and approach shared decision making; troubleshooting attitude; flexibility and creativity; complacency
Organizational issues pre-dialysis; access; financial; and assisted PD
Quotes from respondents have been included in the study to illustrate how these themes were identified and prioritized, which showed there are more intrinsic factors impacting the uptake of home dialysis, compared to the usually reported factors of late referrals, pre-nephrology care, etc.
Learn MoreSpecial PD Edition:
In Case You Missed It! May 2024
This month’s newsletter highlights a selection of recently published peer-reviewed articles featuring peritoneal dialysis (PD).
Peritoneal Dialysis Recent Findings
Assisted peritoneal dialysis: Position paper for the ISPD
Physical, cognitive, and behavioral disabilities are common barriers to self-care PD. Authors highlight situations when assisted PD could help overcome these barriers and expand PD therapy availability to individuals not deemed suitable otherwise. The authors propose a new systematized approach to assisted PD by way of alternative funding models, patient indications, operational models, and payment justifications.
Learn MoreIn Case You Missed It! April 2024
This month’s newsletter highlights a selection of recently published peer-reviewed articles that piqued our interest, grouped by their most relative modality:
Home Hemodialysis (HHD)Peritoneal Dialysis (PD)
We hope you find these recent findings useful and of value in your day-to-day practice.
Home Hemodialysis Recent Findings
Patient Training and Patient Safety in Home Hemodialysis
The authors review the epidemiologic data characterizing the safety of home hemodialysis (HHD) as compared with conventional in-center hemodialysis and how patient training affects safety, while emphasizing the surprising lack of literature surrounding these topics.
Learn MoreIn Case You Missed It! March 2024
This newsletter highlights a selection of recently published peer-reviewed articles that piqued our interest, grouped by their most relative modality.
We hope you find these recent findings useful and of value in your day-to-day practice.
Home Hemodialysis (HHD) Recent Findings
Patient Survival with Extended Home Hemodialysis Compared to In-Center Conventional Hemodialysis
Patient survival, technique survival, hospitalization, and clinical, laboratory, and medication changes were retrospectively analyzed in 349 HHD patients treated with longer session duration, most on nocturnal, were compared to 1,047 concurrent, propensity-score matched in-center hemodialysis patients, using 47 variables with a long-term follow-up.
Learn MoreIn Case You Missed It! February 2024
This newsletter highlights a selection of recently published peer-reviewed articles that piqued our interest, grouped by their most relative modality.
We hope you find these recent findings useful and of value in your day-to-day practice.
Home Hemodialysis Recent Findings
Therapeutic vancomycin and daptomycin levels were analyzed in 5,000 simulated home hemodialysis (HHD) patients. Initial vancomycin and daptomycin doses were defined for 10 common HHD treatment regimens based on HHD treatment duration, days per week, and dialysate volume.
Learn More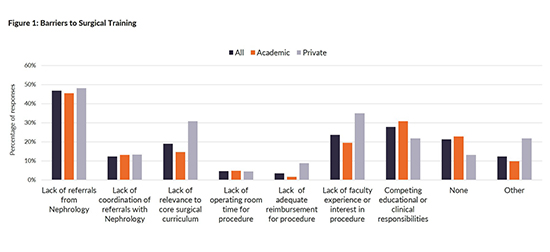
Peritoneal Dialysis Catheter Insertions: Better Outcomes Through Better Communication
“The single biggest problem in communication is the illusion that it has taken place.”–George Bernard Shaw (1856-1950)
Advancing American Kidney Health
While the Executive Order set forth bold goals to increase home dialysis utilization amongst patients with end stage renal disease (ESRD),1 the COVID-19 pandemic has served as an even greater impetus to allow appropriate patients to dialyze at home. In many areas, the cancellation of elective surgeries has led to delays in getting appropriate accesses created for our ESRD patients. For some, timely access creation was an issue even before the pandemic.
Learn More
Peritoneal Dialysis in the Pandemic and Post-Pandemic World
Opinion article
International Practice Considerations After COVID-19
As England moves into the recovery phase from COVID-19, it is worth reflecting on newly enacted changes in clinical practice that should be sustained going forward. This could be particularly helpful to my colleagues in the United States, still in the midst of the pandemic.
In the United Kingdom, when we considered our response to the pandemic, there was heightened concern for those patients requiring dialysis or approaching the need for dialysis.
Learn More
Peritoneal Dialysis in the United States Amidst COVID-19
Opinion article
Clinical Practice Learnings with Potential Post-Pandemic Application
The world is amidst a public health crisis related to the COVID-19 pandemic. COVID-19 will remain a primary healthcare concern until a vaccine and effective medications are discovered, which may take many more months.1 End-Stage Renal Disease (ESRD) patients are at particularly high risk of this coronavirus infection because of chronic immunocompromised state, a high burden of co-morbid conditions, and high healthcare utilization.
Learn More