International Guidelines for Increased Hemodialysis Time and Frequency
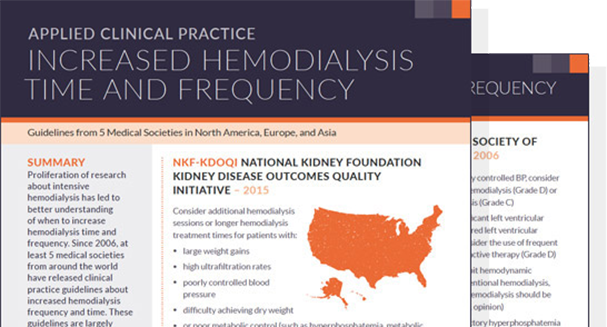
During the past 10 years, there has been a proliferation of research about intensive hemodialysis, including both longer and more frequent hemodialysis sessions. The accumulation of data from studies has led to the development of clinical practice guidelines about hemodialysis time and frequency, with a focus on identifying indications for increasing time and frequency.
In the United States, Medicare requires medical justification for reimbursement of additional hemodialysis sessions (i.e., treatment beyond 3 sessions per week). Clinical practice guidelines not only from the United States, but also from Japan, the United Kingdom, Europe, and Canada together encourage physicians to consider applications of longer and more frequent hemodialysis sessions in patients with cardiovascular complications, including left ventricular hypertrophy and uncontrolled hypertension; hemodynamic instability during dialysis, possibly due to excessive ultrafiltration intensity; hyperphosphatemia; and malnutrition. In fact, relevant clinical practice guidelines are quite concordant in their conclusions about intensive hemodialysis, despite the rapidly evolving base of evidence between the 2006 publication of guidelines in Canada and the 2015 publication of guidelines in the United States.
Applied Clinical Practice Recent Findings
Download PDFThe downloadable document summarizes relevant clinical practice guidelines from around the world, along with years of publication and grades of evidence. Of course, evidence grades must be considered in the context of the mix of relatively small randomized clinical trials and many observational studies of intensive hemodialysis. We will never have randomized clinical trials of intensive versus conventional hemodialysis, with enrollment in the thousands of patients. Thus, physician judgment, coupled with guidelines, is key to identifying patients who, from a clinical perspective, would be good candidates for intensive hemodialysis.